Pleurodesis is a procedure used to treat fluid build-up around the lungs, called pleural effusions, a symptom of pleural mesothelioma. This procedure seals your pleural cavity, the space between the lung and chest wall, which are two thin layers called the visceral and parietal pleura.
Pleurodesis is a surgical procedure used to treat pleural effusions, the buildup of fluid in the space between the layers of the pleura. For people with pleural mesothelioma, this fluid buildup can make breathing difficult and painful. The procedure seals the pleura so that the lung sticks to the chest wall, preventing more fluid from collecting.
Pleurodesis: Key Facts
Pleurodesis is a medical procedure that permanently seals the pleural space, the area between the lung and chest wall, to prevent fluid or air from accumulating.
Doctors most commonly perform pleurodesis to treat recurrent pleural effusions, a buildup of excess fluid that causes shortness of breath, chest pressure and pain.
The 2 main types are chemical pleurodesis, which uses agents like talc to create scar tissue, and mechanical pleurodesis, which uses physical abrasion during surgery.
According to clinical research, talc pleurodesis has a success rate of approximately 80% to 95% in preventing fluid recurrence (National Library of Medicine).
Most patients stay in the hospital for approximately 3 to 5 days after pleurodesis, with full recovery typically taking several weeks.
Doctors don’t use pleurodesis to treat your mesothelioma directly. Instead, it controls one of the most disruptive symptoms of asbestos-related diseases: pleural effusion. According to a 2024 study in Open Respiratory Archives, about 30% of mesothelioma patients receive pleurodesis.
As Sean Marchese, R.N., an oncology writer for The Mesothelioma Center, explains, “Pleurodesis for mesothelioma closes and seals the pleural space in the chest wall where fluid can build up. This technique reduces your risk of pleural effusions, pneumonia and other chest complications.”
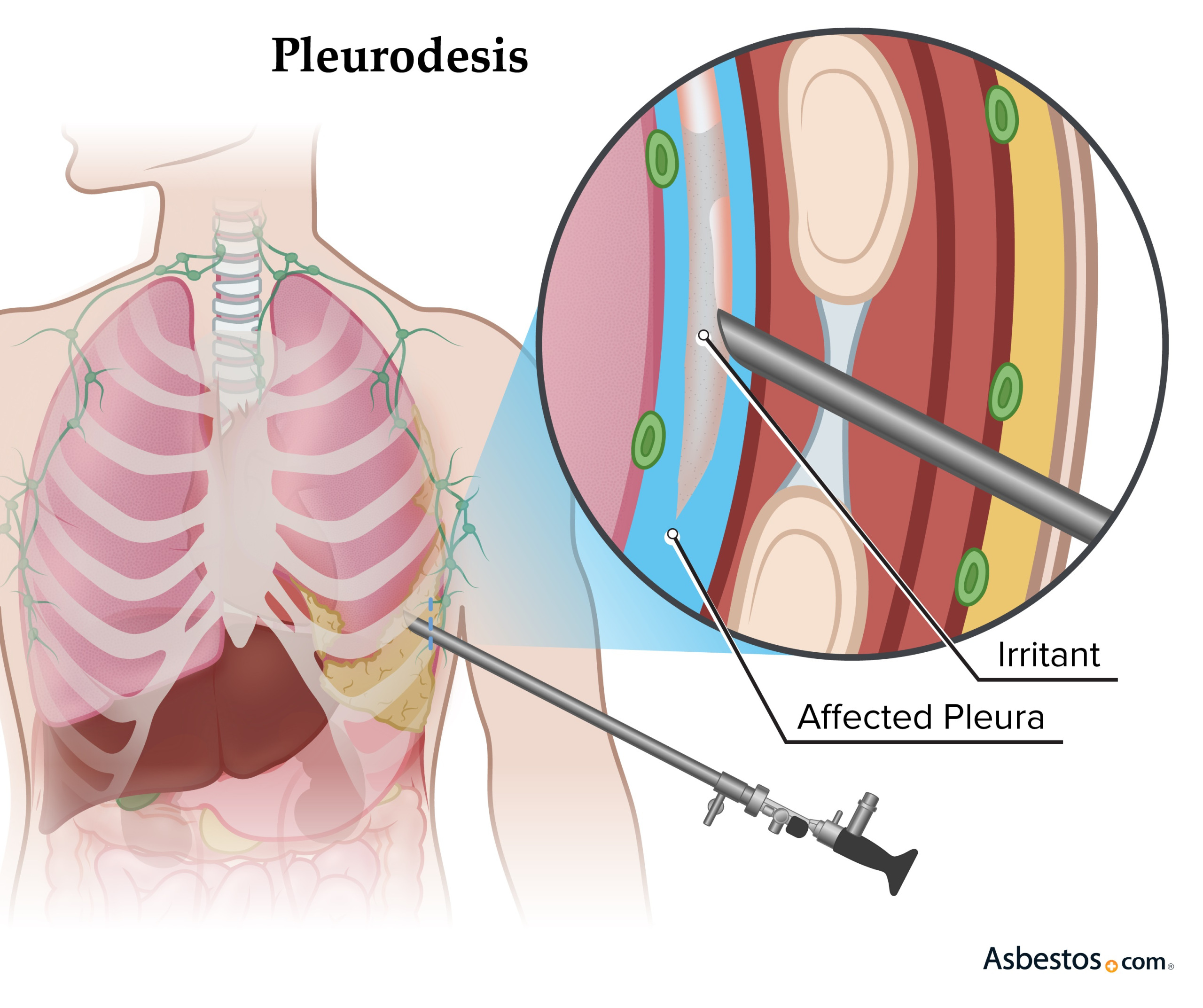
Illustration shows how a pleurodesis seals lining with an irritant.
Types of Pleurodesis Procedures
There are two main types of pleurodesis for mesothelioma patients: chemical and mechanical. Studies have shown similar results between mechanical and chemical pleurodesis. No matter the type, the procedure usually requires about 3 to 5 days in the hospital.
Doctors choose which type of pleurodesis to perform based on a patient’s overall health, cancer stage and treatment goals. Doctors often choose chemical pleurodesis for patients who can’t have surgery, while surgeons typically perform mechanical pleurodesis during another surgical procedure.
Chemical Pleurodesis
Mechanical Pleurodesis
Method
Sclerosing agent injected through chest tube (talc, tetracycline, iodopovidone)
Physical abrasion of pleural surfaces during VATS or thoracotomy
Best for
Patients unable to undergo surgery; malignant pleural effusions
Patients undergoing concurrent surgery; pneumothorax with recurrence risk
Success rate
About 80% to 95% (talc)
Similar effectiveness; varies by technique
Recovery
3 to 5 days hospital stay
3 to 5 days hospital stay; recovery tied to surgical procedure
Anesthesia
Local anesthesia or sedation
General anesthesia
Chemical Pleurodesis
Doctors use agents such as talc (a mineral), tetracycline (an antibiotic) and povidone-iodine (an antiseptic) in chemical pleurodesis for mesothelioma. These ingredients help create the scar tissue needed.
There are 2 main ways to do pleurodesis with talc: poudrage and slurry. Poudrage sprays talc powder into the chest during a small camera procedure called thoracoscopy. Slurry mixes talc with saline and is inserted through a chest tube.
A faster method is rapid pleurodesis, which drains the fluid and delivers the treatment at the same time. It helps you recover quicker and leave the hospital sooner, especially if you’re not healthy enough for surgery.
According to the National Library of Medicine, talc pleurodesis has a success rate of approximately 80% to 95% in preventing the recurrence of pleural effusions. This makes talc the most widely used and effective sclerosing agent, which is a substance used to deliberately cause irritation so inflammation will happen and seal the space. The success rate depends on factors including the patient’s overall health, how well the lung can expand and the volume of fluid present before the procedure.
Mechanical Pleurodesis
Mechanical pleurodesis for mesothelioma is a procedure that uses tools such as gauze or a brush pad to irritate the chest lining. This process causes inflammation and the formation of scar tissue, which creates dry adhesion, making the lung stick to the chest wall.
Surgeons usually do this procedure during a small camera surgery called video-assisted thoracoscopic surgery. Sometimes, VATS is done during a larger surgery called a thoracotomy after removing fluid or air. In some cases, part or all of the lining of the lung (pleura) is removed.
FREE TREATMENT CARE KIT
Ease Your Mesothelioma Treatment Experience
Get a mesothelioma treatment care kit filled with thoughtful items to bring comfort and encouragement while undergoing treatment.
How long your pleurodesis procedure will take depends on the type being performed and the amount of fluid that needs to be drained. Usually pleurodesis takes anywhere from 30 minutes to several hours. Chemical pleurodesis, including rapid pleurodesis, usually takes less time than mechanical pleurodesis.
What to Expect During Pleurodesis
Fluid drainage: First, your doctor inserts a small tube into your chest to remove fluid. This helps your lungs expand. The tube stays for 1 or 2 days until the fluid stops.
Sealing the pleura: After draining fluid, your doctor may add talc or perform a minor procedure to help the lung layers stick together, causing controlled irritation that forms an adhesion. You might feel chest pain, which will be treated with medication.
Hospital stay & recovery: You’ll stay in the hospital for a few days for observation and to manage pain. The tube is taken out once the pleura is sealed. Full recovery can take a few weeks. Your doctor will give you care instructions for home.
Recovery begins in the hospital, but most people go home after 3 to 5 days. Complete recovery may take a few weeks. Your mesothelioma care team or a Patient Advocate can help answer any further questions you may have about the procedure.
Recovery From Pleurodesis Surgery
Recovering from mesothelioma surgery like pleurodesis involves a short hospital stay and then several weeks of rest at home. During recovery, you may have restrictions on lifting or driving and should avoid strenuous activity. Your care team will manage your pain and ensure your lung remains sealed to the chest wall.
You can eat bland foods if your stomach is upset after anesthesia. Your medical team will tell you how long to leave dressings, tape or stitches on. Avoid swimming or baths for 2 weeks. Showering is okay after 2 days, but pat the incision dry.
Who Qualifies for a Pleurodesis?
If you’ve been diagnosed with malignant mesothelioma, you may qualify for pleurodesis if pleural effusions impact your daily life and you can tolerate the procedure. For pleurodesis to work well, your lung needs to expand fully. People whose tumors are so large that their lung can’t fully expand aren’t good candidates for this procedure.
Who May Qualify for Pleurodesis
Patients with fluid in chest that often builds up, needing to be drained once or more each month.
Your expected life expectancy should be at least 3 months.
You should be able to tolerate general anesthesia and long surgeries.
You should be generally healthy.
People with localized cancer who are in good health may also choose a more aggressive treatment, such as pleurectomy/decortication, to remove the tumor. This surgery removes the pleural lining rather than just sealing it. Those who don’t want to undergo hospitalization or recovery from pleurodesis may opt for different palliative treatments for mesothelioma.
In addition to treating pleural effusions from mesothelioma, doctors also use pleurodesis to treat fluid buildup from other cancers. They may also use it for pleural effusions from heart failure, kidney or liver problems, autoimmune diseases and long-term lung issues.
David Doust
Verified Asbestos.com Survivor
Second Pleurodesis Leads to Mesothelioma Diagnosis
Doust’s journey with the asbestos-related cancer began in early 2016 when he experienced shortness of breath, or dyspenea. Wrongly diagnosed with pneumonia, he underwent a pleurodesis to remove excess fluid from around the lungs and was soon back to his exercise routine. Upon returning to Perth, he underwent another pleurodesis. He was told he had acute lymphatic leukemia and pleural mesothelioma.
Pleurodesis offers several benefits for people living with pleural mesothelioma, such as symptom relief and reduced need for ongoing care. Its main goal is to improve quality of life, relieving symptoms.
Key Benefits of Pleurodesis for Mesothelioma
Symptom relief: Helps ease shortness of breath and chest pressure.
Reduced recurrence risk: Prevents pleural fluid from returning.
Reduced hospitalizations: Fewer fluid drainages and emergency visits.
Alternative to ongoing care: May reduce the need for repeated procedures.
Symptom management is an important part of treating pleural mesothelioma. Procedures like pleurodesis help people feel more comfortable as they explore additional treatments that directly address mesothelioma.
I had chest pain when I took a deep breath. I eventually had a biopsy and pleurodesis that provided the definitive diagnosis. Attitude counts for a lot, and willingness to pursue treatment adds up to a better chance for survival.
Jo D., pleural mesothelioma survivor.
Pleurodesis Complications and Risks
The most common risks of pleurodesis for mesothelioma are chest pain and fever. Some people may feel shortness of breath or tightness around the lungs, but medicines can usually help before the procedure.
Fever is frequently associated with the inflammatory response that helps seal the pleural space. It may develop within a few hours of the procedure. In some cases, the procedure may not succeed, leading to incomplete adhesion of the pleural wall spaces.
Risks of Pleurodesis for Mesothelioma
Chest pain
Fever
Infection
Any surgical procedure carries a risk of infection. Generally, a medical team can treat infections with antibiotics. In very rare cases, pleurodesis can cause other complications, such as acute respiratory distress syndrome or cardiovascular complications.
One patient was diagnosed with mesothelioma seven years after undergoing a talc pleurodesis procedure, having had no prior mesothelioma diagnosis. Testing traced his diagnosis to the talc used during his procedure, which was found to be contaminated with asbestos. Talc is a naturally occurring mineral often found near asbestos in the earth. Asbestos can contaminate talc during mining. The patient filed a lawsuit and a jury awarded him $39 million, which a judge later reduced to $23.6 million. If you have concerns about the use of talc in your procedure, speak with your doctor about your options.
Common Questions About Pleurodesis
What is the life expectancy for mesothelioma patients after a pleurodesis?
Life expectancy after a pleurodesis depends on other treatments and health factors. Many patients live for several months to a year or more after pleurodesis, especially when combined with other therapies.
What are the long-term effects of pleurodesis?
The most common long-term effects include mild chest discomfort or occasional shortness of breath. In most cases, pleurodesis successfully prevents fluid buildup without major complications.
Why is pleurodesis used for pleural mesothelioma?
Pleurodesis treats pleural effusions, a common and painful symptom of pleural mesothelioma. It helps reduce shortness of breath and improves comfort.
Is pleurodesis a cure for mesothelioma?
No, pleurodesis doesn’t cure mesothelioma. It’s a palliative procedure that helps manage symptoms. At the moment, there is no cure for mesothelioma.
What type of pleurodesis is best for mesothelioma patients?
The best type depends on your health and cancer stage. Chemical pleurodesis is common, especially for people who can’t have surgery. Mechanical pleurodesis is often used during other surgeries.
How long does a pleurodesis procedure take?
The time it takes to complete a pleurodesis ranges from 30 minutes to several hours. Factors that affect how long it could take include the procedure type and the volume of fluid present. Chemical pleurodesis through a chest tube often takes less time than mechanical pleurodesis during video assisted thoracic surgery or VATS. Patients typically stay in the hospital for approximately 3 to 5 days after the procedure for observation and recovery.
What is the success rate of pleurodesis?
Talc pleurodesis, the most commonly used form, has a success rate of approximately 80% to 95% in preventing the recurrence of pleural effusions, according to the National Library of Medicine. Success rates can vary based on the patient’s health, cancer stage and whether the lung can fully expand. Chemical and mechanical pleurodesis generally show similar effectiveness, though individual outcomes depend on the specific clinical situation.
Recommended Reading
Your web browser is no longer supported by Microsoft. Update your browser for more security, speed and compatibility.
If you are looking for mesothelioma support, please contact our Patient Advocates at (855) 404-4592
Fact Checked
Our fact-checking process begins with a thorough review of all sources to ensure they are high quality. Then we cross-check the facts with original medical or scientific reports published by those sources, or we validate the facts with reputable news organizations, medical and scientific experts and other health experts. Each page includes all sources for full transparency.
Reviewed
Asbestos.com is the nation’s most trusted mesothelioma resource
The Mesothelioma Center at Asbestos.com has provided patients and their loved ones the most updated and reliable information on mesothelioma and asbestos exposure since 2006.
Our team of Patient Advocates includes a medical doctor, a registered nurse, health services administrators, veterans, VA-accredited Claims Agents, an oncology patient navigator and hospice care expert. Their combined expertise means we help any mesothelioma patient or loved one through every step of their cancer journey.
More than 30 contributors, including mesothelioma doctors, survivors, health care professionals and other experts, have peer-reviewed our website and written unique research-driven articles to ensure you get the highest-quality medical and health information.
About The Mesothelioma Center at Asbestos.com
Assisting mesothelioma patients and their loved ones since 2006.
Helps more than 50% of mesothelioma patients diagnosed annually in the U.S.
A+ rating from the Better Business Bureau.
5-star reviewed mesothelioma and support organization.
My family has only the highest compliment for the assistance and support that we received from The Mesothelioma Center. This is a staff of compassionate and knowledgeable individuals who respect what your family is experiencing and who go the extra mile to make an unfortunate diagnosis less stressful. Information and assistance were provided by The Mesothelioma Center at no cost to our family.
Asbestos.com. "Pleurodesis." Last modified April 21, 2026. https://www.asbestos.com/treatment/surgery/pleurodesis/.
Most helpful, steered us in the right direction for treatment. Great source of information and support, the Center followed through on every one of our requests.
Because of their guidance, I was able to navigate getting my mother into MD Anderson when her case got put aside by mistake in all the COVID-19 craziness. Vanessa was amazing and I can’t recommend enough reaching out to them. I thought it was a gimmick to get you to hire a lawyer, but I was so wrong. They truly seemed to want to help meso patients and KNOW what you need to ask and do in order to get help.
Hearing the news about my mother's diagnosis was heartbreaking. I felt lost, I didn't know how I could help or where to seek the best medical care. I started researching specialists online and shortly after, Dr. Smart reached out to me. She has been extremely helpful and encouraging throughout this entire process. Even though we aren't located in her area, she has helped us get in contact and set up appointments with the best doctors/specialists nearby. She has always been available for any questions that we have, and she even sent us a binder full of helpful resources. The patient advocates are amazing and true to their title. Dealing with this process is not easy, but knowing that we have someone like Dr. Smart in our corner is reassuring and we are so grateful for her and The Mesothelioma Center.
My son Carlos was diagnosed with this terrible and unknown disease a few months ago. Thank God we found The Mesothelioma Center along the way, and Vanessa Blanco who provided us with information on hospitals and doctors who have been of great help. I am very grateful to them.
Extremely communicative and helped my dad get an appointment with one of the top centers in Philadelphia. I'm so grateful for this center. They assisted with information on nutrition, legal help, and scheduling appointments. Special thanks to Danielle!
Danielle DiPietro was an invaluable resource for me. Her suggestions and recommendations guided us towards stellar practitioners in our area. Without her advocacy, I feel we would have been receiving less-than-optimal medical and legal care for mesothelioma. Receiving the diagnosis was a shock and I felt lost initially. I wish everyone could take advantage of this FREE assistance.
I was very grateful and appreciative of Dr. Smart from The Mesothelioma Center. She was very helpful to my husband and me. She educated and walked us through the steps, and suggested ideas and questions to ask his doctors. She also provided me with a lot of information that I can read and educate myself about this illness. We need more people like Dr. Smart, who is very educated and you can tell she enjoys the work that she does by the way she assisted my husband and me. We thank the Lord and are grateful that we met Dr. Smart from The Mesothelioma Center.
In January of 2016, my husband was diagnosed with peritoneal mesothelioma. Our first reaction was: what is this and what can we do? He was diagnosed by an oncologist and was scheduled to start chemotherapy. When we arrived home that day, I googled mesothelioma and discovered The Mesothelioma Center had a form to fill out to request additional information. I filled it out and within an hour, I received a phone call from Karen Selby from The Mesothelioma Center asking if I needed any help. Karen was and still is my lifeline. She located a doctor at the Cleveland Clinic who performed surgery and HIPEC on peritoneal mesothelioma patients. My husband was scheduled with an appointment and his surgery was performed on March 3, 2016. He continued with follow-up appointments with the oncologist until a friend of ours passed away from it in 2017. Immediately I sent Karen an email asking if she knew any mesothelioma specialists at the clinic, and of course, I got a prompt response back with a name. Everything was going well until the last CAT scan, which showed it returned. He is now doing chemo and has his next CAT scan scheduled for the end of March with a follow-up for the results with the mesothelioma doctor. Without Karen, I am not sure my husband would still be here. She provided me with so much information along with help in various ways, too numerous to even mention. Thank you to all those who are there to help us.
Dr. Jacques Fontaine is a thoracic surgeon at Moffitt Cancer Center in Tampa, Florida, where he heads up the Mesothelioma Research and Treatment Center. He specializes in minimally invasive robotic surgery and aggressive surgeries for mesothelioma.
Fact-checked and verified content:
Our fact-checking process begins with a thorough review of all sources to ensure they are high quality. Then we cross-check the facts with original medical or scientific reports published by those sources, or we validate the facts with reputable news organizations, medical and scientific experts and other health experts. Each page includes all sources for full transparency.
Please read our editorial guidelines to learn more about our content creation and review process.